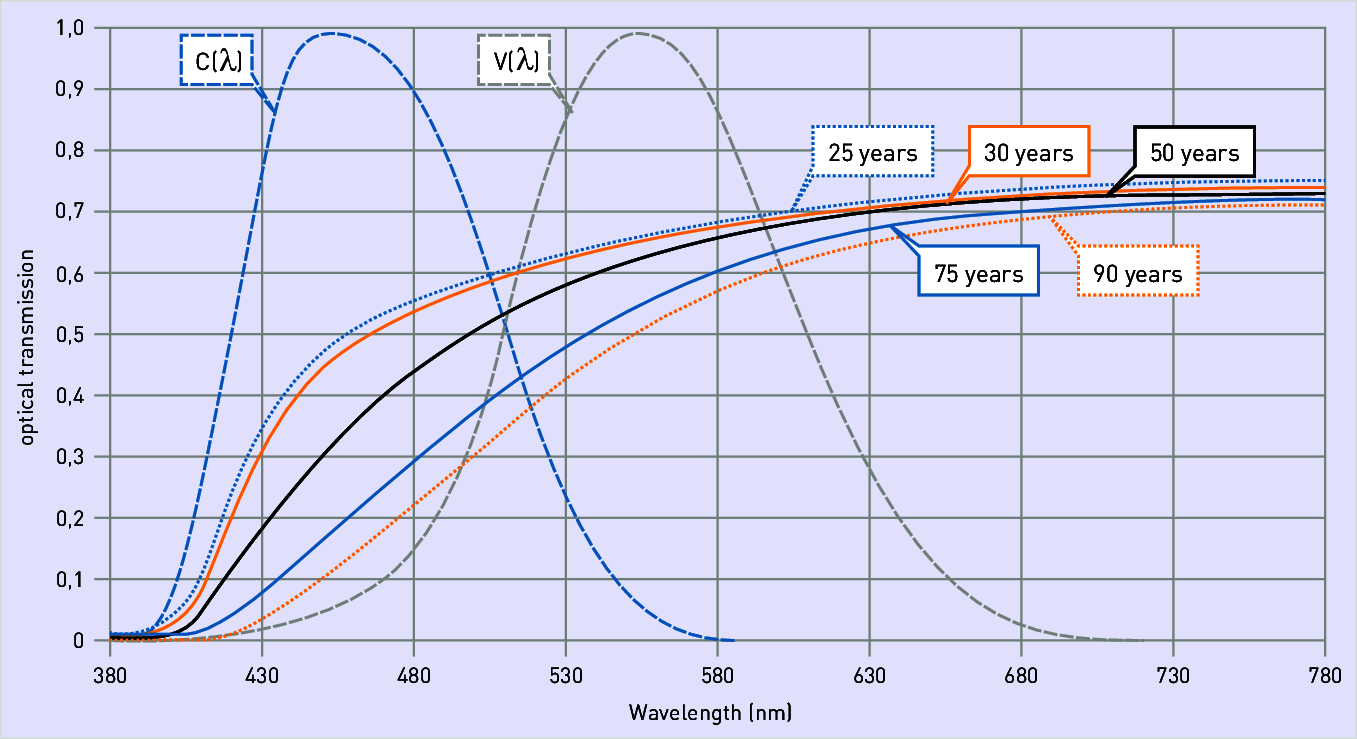
Figure 3.139: Age dependency of lens clouding compared to luminous efficiency
Postbox 1960
D-59753 Arnsberg
Figure 3.139: Age dependency of lens clouding compared to luminous efficiency
Older people have significant issues with limited blue light perception (figure). Compared to a 30-year-old, only ca. 20% of blue spectral components reach the retinal ganglions, which regulate the biological (circadian) rhythm and thus melatonin levels, in a 75-year old due to yellowing of the lens (see also chapter "Light and health"). The consequences are behavioural disorders during the day and sleep disorders at night. Due to frequent walking impairments, the people in question also tend to go outside less frequently or not at all. They live predominantly indoors and in "biological darkness" – meaning with lighting featuring insufficient illuminance and insufficient colour variation.
Due to the distribution of blue receptors in the lower retinal area, light with an elevated blue component, e.g. at a colour temperature ≥ 6.500 K hitting the eye from the ceiling or upper wall areas has a more efficient melanopic (non-visual) response than light from lower areas of the field of vision (figure).
Figure shows the result of a study with Alzheimer's patients who spent most of their time in predominantly artificially illuminated indoor spaces. The initial situation shows a disordered waking and sleeping pattern: at night time, patients were often active while being sleepy during the day. Upon prescriing melatonin medication, the day/night rhythm normalised. Once the melatonin administration was discontinued, disorders in the waking and sleeping rhythm became apparent once more. This leads to the conclusion that treatment success must also be achieved through natural melatonin production or suppression in the body. Trials in geriatric care homes with light ceilings controlled analogously to daylight have confirmed this. Limited stays of as little as a few hours per day spent under a light ceiling with high illuminance (ca. 1.500 lx) at a colour temperature of 6.500 K (daylight) compensated for typical daylight deficiency symptoms and relieved day/night rhythm disorders in the senior residents (see also chapter "The melanopic efficiency of light").
This leads to the recommendation for providing a special lighting installation in certain areas of geriatric care or nursing homes, e.g. in common rooms or other occupancy areas. Direct-indirect-distribution luminaires or a light ceiling, for example, can dynamically control lighting level and light colour – aligned with daylight – and can be utilised for limited amounts of time in order to synchronise the circadian rhythm (e.g. for two hours during the day). This type of treatment provides a long-term effect: interruptions of up to 2 weeks have insignificant effects on the day/night rhythm once it is soundly synchronised. Light ceilings (figure) can be set over a wide range for this purpose: from activating lighting with up to 2.800 lx and 6.500 K down to comfort lighting at e.g. 500 lx and 2.700 K. Lighting systems of this type may not exactly replicate natural daylight, but they do achieve a certain proximity in terms of characteristics.
In a city in the south of Germany, vertical illuminance and vertical colour temperature of daylight were measured in a northward direction (meaning without direct solar irradiation) on 1 May (see table). The values show that light ceilings are absolutely capable of imitating the positive biological effects of natural daylight.
At this point in time, there are many studies available in which normally adjusted waking and sleeping behaviours were observed after some time under lighting with this kind of control mechanism, similar to results achieved in melatonin medication (figure). Beyond that, depression was alleviated, aggression was reduced and states of dementia were mitigated.
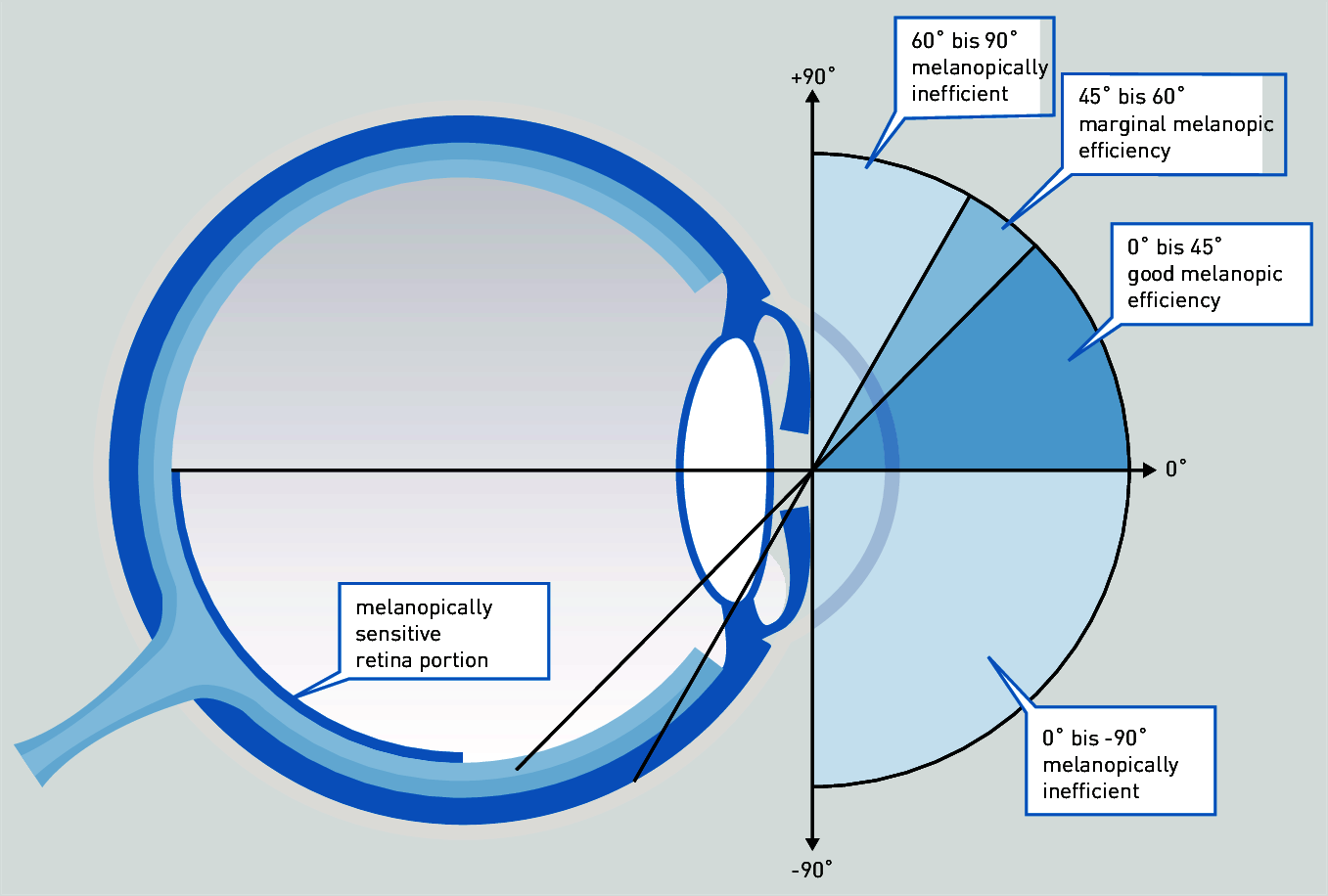
Figure 3.140: Blue light incident on the eye within the range of 0° to 45° achieves the strongest melanopic efficiency
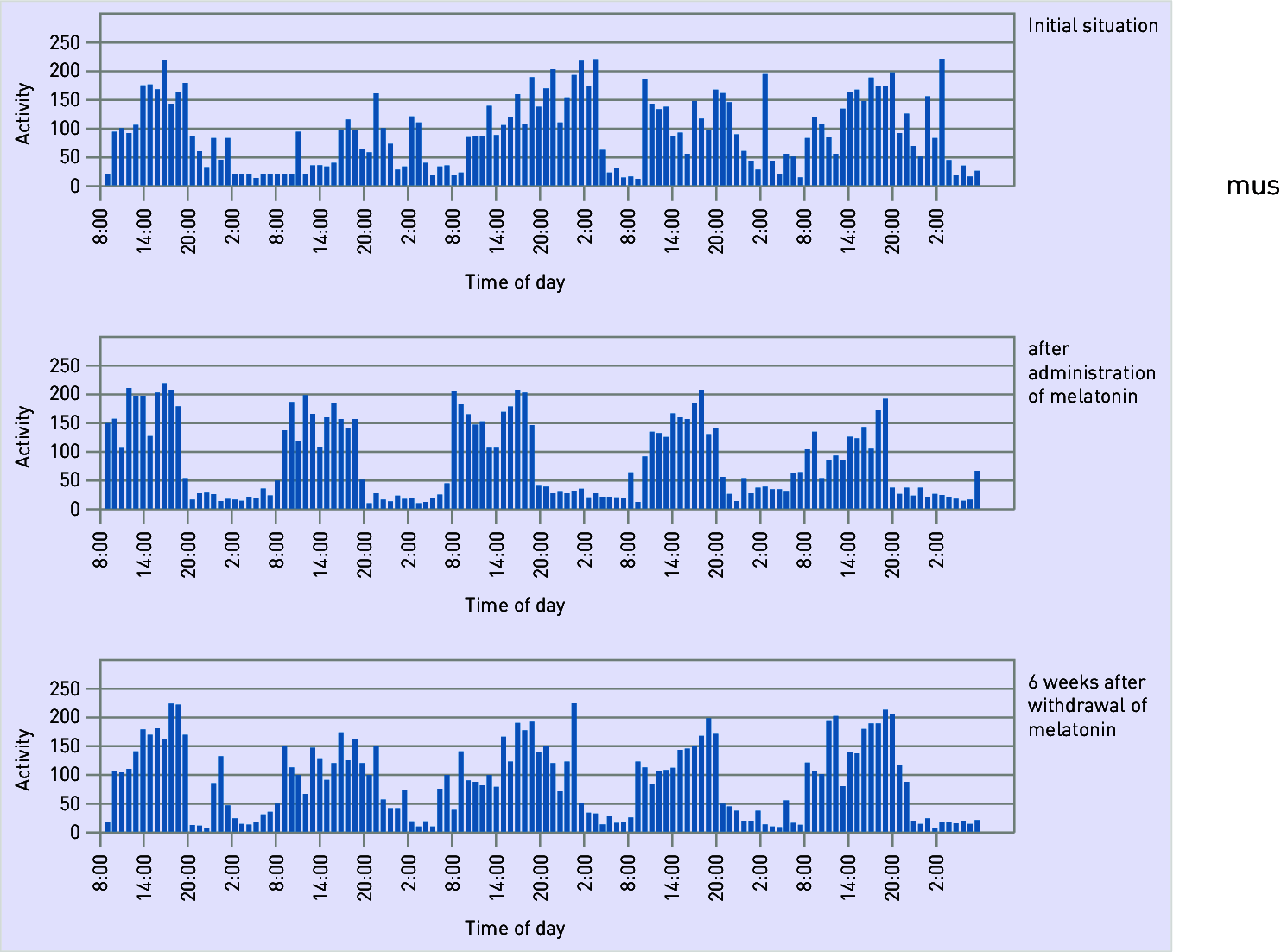
Figure 3.141: Melatonin treatment success in Alzheimer's patients relating to day/night rhythm